Why Knowing Pain Type Matters
We all experience uncomfortable, sometimes painful sensations in our soft tissues from time to time. This happens either after physical activity, but can also be the result of sitting for long periods of time. Less often, these sensations can become compulsive, recurring from time to time and we realize that something needs to be done about it. Exercise and going to a massage therapist often solve the problem. And yet, fortunately, relatively rarely, these sensations can escalate into real pain and already seriously bother us.
To figure out what to do about it, it is advisable to identify the specific tissues implicated in the discomfort or pain. This determination facilitates informed decisions regarding subsequent steps, whether they entail revisiting a massage therapist or consulting a medical professional.
The inquiry into the specific tissue involvement consistently emerges for the massage therapist whenever a client presents with complaints of soft tissue pain. Once the massage therapist understands what exactly is involved, he or she can correctly build the tactics of massage and determine the overall strategy – give adequate recommendations, advise the necessary exercises or justify the need to visit a doctor for further examination.
Mechanism of pain formation
Even with a rudimentary comprehension of the mechanisms underlying pain sensation, one can gain insight into the structures from which it originates. Two main mechanisms of pain can be distinguished: Nociceptive pain and Neuropathic pain.
Nociceptive pain
The formation of pain sensations begins with special pain receptors. These receptors are located in almost all tissues of the body and can respond to mechanical and thermal effects, as well as to chemical changes in the surrounding tissues.
The impulses then travel along afferent neurons (which form the basis of nerves) to the Central Nervous System. (CNS). The path of nerve impulses can vary from a very short reflex arc in the nearest spinal cord segment (like pulling away a finger that touches a hot object) to a long arc to the different structures of the brain.
We won’t get into all the details to keep things short.
The mechanism described above is shown in Fig. 1. Receptors in the injured tissues (shown in red) conduct pain impulses to the CNS.
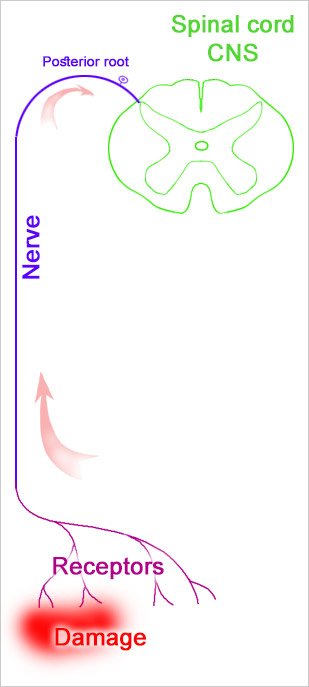
Such a mechanism of formation and conduction of nerve impulses is universal for the organism. Other types of sensitivity use exactly the same scheme. The nerves themselves remain uninvolved in the pathological process. Pain arising from such conduction of impulses is called Nociceptive pain.
Neuropathic pain
In contrast to the above, there is another mechanism of pain in which the nerve itself is damaged while the soft tissues remain intact. This is called Neuropathic pain
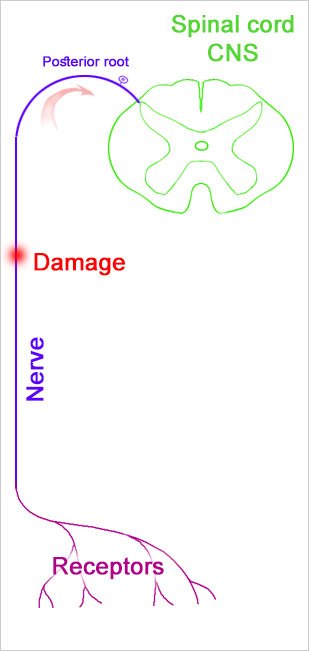
Let’s look at the events that occur in this pain mechanism (Fig. 2). Pain impulses originate in the area of the nerve damage. The CNS perceives these impulses as coming from receptors. Note that receptors can be located far from the site of nerve damage. That is, a person may feel pain not in the area of the nerve damage, but in the area of nerve endings
Key Differences in Pain Characteristics
The structural differences in the pain mechanisms described above appear to determine the differences in symptomatology as well, allowing us to distinguish soft tissue injuries from damage to the nerves themselves.
Nociceptive pain
Nociceptive pain is usually local and not radiating. Depending on the extent of tissue involvement, the characteristics of the pain will vary from aching to dull. The intensity is usually low to moderate.
Neuropathic pain
Neuropathic pain produces a wide range of symptoms. By nature, the pain is sharp, pulsating, stabbing or burning, sometimes resembling an electric shock, often radiating along the course of the nerve. The pain can be quite intense. Because different nerve fibers are involved, other symptoms such as numbness, tingling, local loss of sensation and, in prolonged cases, muscle atrophy may also be observed. Touching the skin in the area of nerve innervation can become very painful.
Examples
So-called Thoracic outlet syndrome (TOS) in which the nerve fibers are affected in the neck area (often simply compressed by tense neck muscles). In this case, numbness and tingling sensations can be felt in the fingers. Pain can be anywhere in the arm, often in the fingers or elbow. Sometimes shooting pains can be felt along the entire arm.
In Sciatica, the nerve may be compressed in the lumbar vertebrae or by the pelvic pear muscle. In this case, the sensation can be felt along the back of the leg down to the heel.
Simple Tools to Help You Tell the Difference
painDETECT
PainDETECT was first introduced as a diagnostic tool tailored specifically for individuals dealing with persistent lower back discomfort. More about PainDETECT on Phyisiopedia.
DN4
The Douleur Neuropathique en 4 Questions (DN4) is a validated screening tool developed in 2003 by a team led by Didier Bouhassira to help clinicians identify neuropathic pain. It’s widely used in both clinical and research settings and has become a gold standard in pain diagnostics.
The application of this information to the massage therapist’s practice
In the course of recognizing the source of pain, the massage therapist must strictly adhere to the routine of an orthopedic assessment. During the history collecting, the exact localization of pain and all other sensations of the client is established. It is worth asking the client to outline the painful area with a finger.
The nature of the client’s complaints already allows us to suspect the involvement of the nerve in the pathological process: sharp, pulsating, electrical pain; the presence of numbness and tingling. All these areas should be described. Different sensations can have different localization. For the convenience of further analysis, it is worth putting them on the scheme of the human body.
The examination includes a standard determination of the type of affected tissue using active and passive movements as well as isometric contraction (A-P-R).
Palpation is important. If nerve involvement is suspected, the massage therapist should palpate not only the areas where the pain is felt but also the entire available path of the nerve.
The area of skin innervation is also examined to determine hypersensitivity in the area of nerve receptors.
For less experienced in anatomy, it is convenient for masseurs to have a diagram of the main nerves, which is worth working with beforehand to make it easier to navigate.
The innervated muscles should also be examined for atrophy (if the nerve has motor fibers).
In case there are difficulties in diagnosis (traditionally massage therapists have little training in diagnosis) it is necessary to methodically and consistently record all the findings, put everything on the schemes, and after the session work through the data with the necessary literature and anatomical atlases and programs.
It is good practice to write up a detailed report describing the symptoms, and findings and add an analysis of potentially involved nerves. This will allow all data to be saved for future massage sessions.
Notes. This is an outline for the self-education of clients and massage therapists. The material is brief, thesis-based, and designed for elementary education. Clients can get a basic understanding of the topic, massage therapists can update their knowledge. This material should not be used as a guide for self-treatment.
ADVERTISING
Evidence-Based Massage in Calgary SE – No Guesswork, Just Results
At Andrew Sague Massage Clinic in Chaparral (Calgary SE), every treatment is based on scientific research and clinical data. I do not use unproven theories or trends. My approach is focused, professional, and backed by real results. If you want massage therapy that works, book today.