Preface
Originally, I planned to write a full-length article. However, that would require more time than I have, and it might be challenging for a non-professional to read and comprehend. So, I decided to focus on concise points, resembling a summary rather than a detailed article. This approach is quicker to write, easier to read, and makes the main ideas clearer.
What is the problem with myofascial adhesion?
The concept of myofascial adhesions is widely discussed in massage literature. It’s believed that these adhesions can be diagnosed and treated through myofascial techniques. Some authors, instructors, and practitioners claim to find adhesions almost everywhere, in nearly every muscle they examine.
Given the widespread use of the term “myofascial adhesion,” one would expect that this condition is well-studied and thoroughly described in specialized literature. However, that’s not the case. The term is often mentioned without a detailed explanation, leaving many massage therapists either unclear about what it truly means or interpreting it in their own way.
There are no significant scientific studies on the morphology (histological structure) of adhesions, the mechanisms behind their formation, or their consequences. The literature offers only vague suggestions that adhesions may limit muscle function and should break up.
Most practicing massage therapists can’t even clearly explain what exactly is adhering to what.
What is adhesion in general?
In a general biological sense, adhesion refers to the fusion of two adjacent tissues that normally shouldn’t stick together. To prevent this, Mother Nature uses a barrier of epithelial tissue (see Fig. 1).
The epithelium is a layer of tightly connected cells that covers the surface of an organ or anatomical structure . For instance, the abdominal and pleural cavities are lined with epithelium. This epithelial lining in the abdominal cavity prevents the intestines from sticking to each other or the abdominal wall. However, if the epithelial layer is damaged by trauma or surgery, adhesions can form.

Muscle fasciae and their interactions.
Let’s examine how the fasciae of two contracting muscles interact.
It’s important to remember that fascia, as a type of dense regular connective tissue, is constantly renewed: cells are replaced, and new fibers and intercellular matrix are produced.
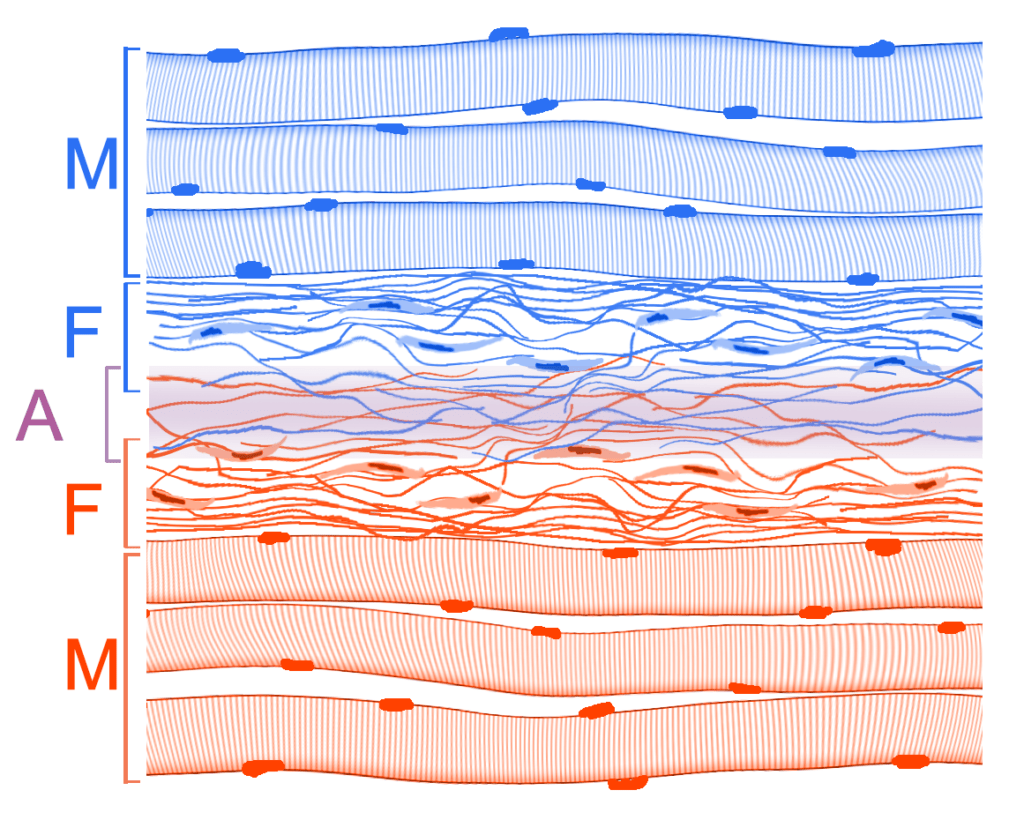
Since there is no barrier like epithelium between the muscles, nothing prevents the connective tissue fibers of one fascia from penetrating into each other (see Fig. 2).
A similar process occurs in a wound with edges connected by surgical sutures. Over time, fibers from one edge grow into the neighboring edge, gradually merging to form a single cohesive tissue.
Therefore, strictly speaking, the term “adhesion” does not apply to fascia, as their continuous fusion is a normal physiological process.
A logical question arises: why don’t muscles grow together into a single entity? The answer is simple and evident—they do fuse, but only up to a certain point.
The limit is set by the muscles themselves through their contraction. When muscles contract, the sliding motion helps to remove excess connective tissue fascial fibers.
Current popular theories suggest that fascia might deform muscles or limit their function. However, these claims are not supported by scientific research.
Fascia, its functions, and strength properties.
Fascia is a thin, almost microscopic layer of tissue. It mechanically protects the superficial muscle fibers and, due to the semi-liquid components of the matrix, provides lubrication to reduce friction.
Fascia also helps to anchor vessels and nerves to the surface of the muscle. This is a general biological function of connective tissue.
However, it is quite naive to think that fascia can limit a muscle’s function. It’s like trying to secure train carriages with shoelaces, hoping the laces will hold them together while the train is moving.
Special cases of fascia damage.
In some severe pathological conditions, a layer of scar tissue may form between the muscles, involving the fascia.
Such processes may include, for example, muscle trauma with rupture of muscle fibers and the formation of intermuscular hematomas, or severe, sometimes purulent inflammation of a muscle area (myositis).
In severe inflammation and under the influence of biologically active substances, a thick layer of fibrous tissue forms. This layer differs from normal fascia and can indeed disrupt normal muscle function.
Such conditions, especially during the acute phase, are rarely encountered by massage therapists, as they are typically treated by medical specialists.
These conditions are well-known in medicine, thoroughly described, and are effectively treated with methods developed long before the advent of myofascial manipulation.
There is still no clear evidence that myofascial manipulation has any effect on such severe disorders or provides any treatment benefits. Therefore, the claims made by proponents of myofascial release are not supported by scientific evidence.
Diagnostics and methods of myofascial intervention.
If you have read this far, you should understand that the term “adhesion” is imprecise and lacks scientific support.
However, to better understand the issue, let’s assume that adhesions do exist. We can then examine the diagnostic and treatment options proposed by proponents of myofascial release from this perspective.
The diagnosis of adhesions involves assessing the restriction of skin mobility over the muscle by shifting it during palpation. It is expected that, in the presence of adhesions, the mobility of the skin and underlying soft tissues will be restricted.
It remains unclear how the presence of adhesions specifically causes limited skin mobility, as the literature does not provide a clear description of the process. Based on discussions in myofascial release courses and with practitioners, it seems the focus is on assessing the mobility of the so-called superficial fascia.
Note that modern anatomical nomenclature no longer includes the concept of superficial fascia. However, for the sake of argument, let’s assume that the superficial fascia does exist.
So, can the adhesion of the (non-existent) superficial fascia be determined by skin displacement? No, it cannot, as such displacement is influenced by many factors unrelated to the fascia.
Two key points can be highlighted.
1. The thickness and elasticity of the subcutaneous fat layer can vary. Due to its mobility, this layer can mask any restrictions in the underlying tissues.
2. The elasticity of the skin itself differs in various directions. This phenomenon has long been recognized by anatomists and surgeons and is well documented. For example, there are various schematics of skin mobility, such as the lines of Langer, Kraissl, RSTL (Relaxed Skin Tension Lines), and others.
The connection between the (now non-existent) superficial fascia and skeletal muscle is also unclear, as skeletal muscle is covered by a completely different layer of fascia—the deep fascia.
There is no clear answer on how to determine adhesions between the fascia of deep muscles. For instance, how would one assess adhesions between the rhomboid major and the iliocostalis thoracis muscles, considering that the rhomboid is covered by the trapezius muscle?
About treatment
The therapeutic effect of strong pressure with tissue displacement—which forms the basis of myofascial manipulations—seems rather questionable, even if we assume the presence of some adhesions.
Connective tissue fibers are quite elastic, so a significant displacement would be needed to tear them. It is much easier, as mentioned above, to induce muscle contraction. In this case, the fibers that restrict muscle contraction will break, while those that do not interfere will remain intact.
Such fibers can be observed during muscle dissection: when muscles are mechanically separated, thin connective tissue bridges are clearly visible between them.
Note that these bridges are easily torn when muscles are pulled apart, without requiring any significant muscular effort. It remains unclear how they could restrain or limit muscle function, as proponents of myofascial release suggest.
It is also unclear how to influence the deep muscles, as neither compression nor skin shifting can provide sufficient displacement. The literature on myofascial release does not address this issue, nor does it discuss the impact on the fascia of deep muscles. Consequently, there is no scientific evidence supporting the effectiveness of such an approach.
After several decades of intensive research into myofascial release, no evidence of adhesions has been presented, their structure remains undetermined, and there is no justification for their treatment.
ADVERTISING
Professional Massage in Calgary SE – No Pseudoscience, Just Results
At my clinic in Chaparral, Calgary SE, I focus on effective, evidence-based massage therapy. I do not use unproven theories like myofascial adhesions. Every technique is backed by scientific research and real clinical results. If you’re looking for real relief—not myths—book your massage today.