Why Using the Term “Fascia” Without Specification Is Incorrect
Every time a massage guru, whether in a video, at a seminar, or in an educational article, uses the word “fascia” in a general sense, without a clarifying definition, it is a reason to be cautious.
From the standpoint of anatomical nomenclature and proper professional language, such generalized usage is incorrect and leads to misunderstanding and errors.
When speaking about fascia, it is correct to specify which fascia is being discussed. As a rule, a modifier is used—most often related to a particular muscle: for example, the gluteal fascia. Some fasciae have their own established names, such as the thoracolumbar fascia or the fascia lata. These are specific anatomical structures with defined locations and functions.
When the word “fascia” is used without clarification, less experienced students and practitioners may develop a distorted understanding of a single, unified fascia as a structure independent from other tissues—essentially as a separate organ. This is precisely the impression that proponents of certain fascial concepts often seek to create: it becomes easier to operate with vague terms, replace strict anatomy with metaphors, and mask methodological weaknesses.
The Terminological Problem of “Superficial Fascia”
In such discussions, “fascia” often implicitly refers to the superficial fascia—but without clarifying that it is specifically the superficial fascia. This is fundamentally incorrect, as the context often makes it unclear what exactly is being discussed.
Meanwhile, in contemporary anatomy, the very concept of superficial fascia is considered methodologically problematic and has been excluded from anatomical classification.
As a result of such careless use of the term, beginners form the impression that somewhere in the human body, between the skin and the muscles, there exists a distinct “fascia.” They are then led to believe that this “fascia” can deform, form adhesions by sticking to muscles, and thereby significantly restrict muscular function. It is also claimed that this supposed fascia can become dense, “shorten,” or even possess contractile properties, literally “binding” the body.
Within such a framework, the role of the massage therapist appears both simple and extremely important: one must identify these restrictions and adhesions, apply special techniques (myofascial release), and free the person from the “grip” of this insidious fascia. The concept is coherent, elegant, and convincing.
The only problem is that it does not correspond to reality—in other words, it is false. Why? Because it is more convenient and easier to sell this kind of pseudo-knowledge. Based on false concepts, it is easy to construct an equally false theory, and from that theory, build courses, modalities, tools—in short, an entire commercial arsenal. And it is not easy to sort out what exactly is wrong with it.
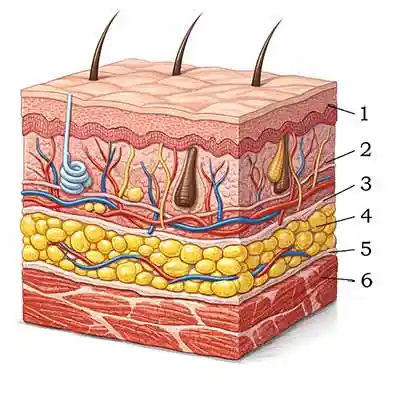
Here is a typical schematic illustration of the skin and underlying tissues without excessive detail. The layers are numbered. Try, without looking at the answers, to indicate which numbers correspond to what you understand as “superficial fascia.”
Answers:
1 — Epidermis.
2 — Dermis.
3 — An anatomically ill-defined connective tissue layer, most likely representing the reticular layer of the dermis gradually transitioning into the subcutaneous tissue (hypodermis).
4 — Hypodermis (subcutaneous tissue).
5 — Epimysium.
6 — Skeletal muscle.
Thus, what is referred to as “superficial fascia” corresponds to the hypodermis (4). Since this layer already has an established name and well-defined functions, duplicating terminology is hardly appropriate — a point that has been reflected in the most recent anatomical nomenclature.